Have you ever wished for the safety of bonds, but the return potential of common stocks? If so, preferred stocks are potentially a good choice to explore.
Real Estate Investment Trusts (REITs) are one of the most dividend-rich segments of the financial market. Understanding the lease structure of commercial REITs can help you identify optimal investment opportunities to include in your portfolio.
Commercial REITs give investors exposure to income-producing real estate in the form of offices, apartment buildings, warehouses, shopping centers and hotels, among others. Commercial real estate leases are generally broken down into three basic categories, which are based on two rent calculation methods: net and gross.
A gross lease requires the tenant to pay one lump sum for a rental property from which the landlord deducts expenses. A net lease has a smaller rental rate but requires the tenant to pay for other expenses.
Click here to learn more about the different types of REITs.
Gross Lease
Under a gross lease, the rent is all-inclusive, which means the landlord pays for all or most of the expenses associated with the property. This includes taxes, insurance, maintenance, utilities and janitorial services. A gross lease offers predictability for the tenant because they can forecast expenses without worrying about unexpected costs like maintenance. Under this arrangement, the landlord assumes all responsibility for maintaining the building.
Net Lease
In a net lease, the tenant is charged a lower base rent for the commercial space and is also on the hook for some or all of the associated costs. These costs often include real estate taxes, property insurance and common area maintenance items. Net leases are broken down into three sub-categories: single net lease, double net lease and triple net lease. Below is a breakdown of each.
Single Net Lease: Tenant pays base rent plus a pro-rata share of the property tax, utilities and janitorial services. The landlord pays all other building expenses.
Double Net Lease*: Tenant pays rent plus a pro-rata share of property tax and insurance, as well as janitorial and utility expenses. The landlord pays for repairs and common area maintenance.
Triple Net Lease: Tenant pays all or part of the property taxes, insurance and common area maintenance on top of a base monthly rent. These tend to be more landlord friendly as they ensure predictability, which can help landlords better manage expenses down the road.
Modified Gross Lease
To bridge the two calculation methods, there’s something called a modified gross lease. While similar to the gross lease in that the rent is requested up front in one lump sum, it can include any or all of the associated “nets,” such as property taxes, insurance and common area maintenance. For most buildings, utilities and janitorial services are excluded from the rent and covered by the tenant. The modified gross lease has proven to be more popular with tenants because it provides greater flexibility.
Use the Dividend Screener to find high-quality dividend stocks. You can even screen stocks with DARSratings above a certain threshold.
Implications for Investors
For investors, REITs with a triple net lease structure are easier to predict in terms of dividend payment. This makes them more attractive for yield-seeking investors, especially those nearing retirement or looking for steady income growth. STORE Capital (STOR ) is one of the most notable triple net REITproviders. The company focuses primarily on fragmented subsectors of the leasing industry, including middle-market and larger companies that don’t have credit ratings. As of 2017, STORE’s leadership team had invested more than $12 billion across 8,000 properties.
REITs structured around single or double net leases also make good investments. For example, W.P. Carey(WPC ) is a global provider of net lease REITs focused on long-term, sale-leaseback and build-to-suit financing solutions.
Realty Income (O ) is a net lease REIT that offers diversification across tenants, industry and geography. By the end of 2017, Realty Income had a portfolio of nearly 250 commercial tenants across 47 industries. It has also proactively managed rollover, including a 99.5% recapture (i.e., re-leasing prior rent).
Although REITs offer tremendous dividend-earning potential, they are highly sensitive to economic cycles and real estate dynamics. Historically, they have underperformed the market during periods of rising interest rates. As we’ve seen during the Federal Reserve’s latest rate-tightening cycle, higher borrowing costs have already impacted the market negatively. Investors should also pay attention to upfront fees, which tend to be exorbitant for non-traded REITs that might require an upfront fee of between 9 and 15%.
Don’t forget to read this article to learn more about how a REIT is valued.
The Final Word
Net lease REITs with long-term leases can provide your portfolio with a sense of stability and transparency. As the previous discussion illustrated, the triple net lease structure offers the most predictability for investors looking for stable earnings over long durations.
U.S. financial services giant Morgan Stanley is buying Calgary-based Solium Capital Inc. for $1.1-billion in the latest deal that will wrest a sizable technology player from Canadian control.
I was working at the Apple Store and I wanted a change. To start building the tech I was servicing.
I began looking into Machine Learning (ML) and Artificial Intelligence (AI).
There’s so much going on in the field.
Every week it seems like Google or Facebook are releasing a new kind of AI to make things faster or improve our experience.
And don’t get me started on the number of self-driving car companies. This is a good thing though. I’m not a fan of driving and roads are dangerous.
Even with all this happening, there’s still yet to be an agreed definition of what exactly artificial intelligence is.
Some argue deep learning can be considered AI, others will say it’s not AI unless it passes the Turing Test.
This lack of definition really stunted my progress in the beginning. It was hard to learn something which had so many different definitions.
Enough with the definitions.
How did I get started?
My friends and I were building a web startup. It failed. We gave up due to a lack of meaning. But along the way, I was starting to hearing more and more about ML and AI.
“The computer learns the things for you?” I couldn’t believe it.
I stumbled across Udacity’s Deep Learning Nanodegree. A fun character called Siraj Raval was in one of the promo videos. His energy was contagious. Despite not meeting the basic requirements (I had never written a line of Python before), I signed up.
Three weeks before the course start date I emailed Udacity support asking what the refund policy was. I was scared I wouldn’t be able to complete the course.
I didn’t get a refund. I completed the course within the designated timeline. It was hard. Really hard at times. My first two projects were handed in four days late. But the excitement of being involved in one of the most important technologies in the world drove me forward.
Finishing the Deep Learning Nanodegree, I had guaranteed acceptance into either Udacity’s AI Nanodegree, Self-Driving Car Nanodegree or Robotics Nanodegree. All great options.
I was a little lost. “Where do I go next?”
I needed a curriculum. I’d built a little foundation with the Deep Learning Nanodegree, now it was time to figure out where I’d head next.
My Self-Created AI Masters Degree
I didn’t plan on going back to university anytime soon. I didn’t have $100,000 for a proper Masters Degree anyway.
So I did what I did in the beginning. Asked my mentor, Google, for help.
I’d jumped into deep learning without any prior knowledge of the field. Instead of climbing to the tip of the AI iceberg, a helicopter had dropped me off on the top.
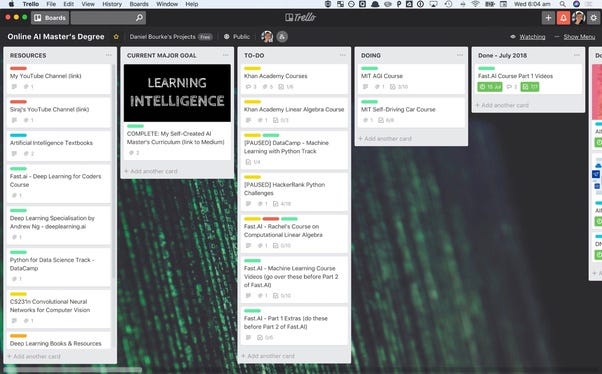
After researching a bunch of courses, I put a list of which ones interested me the most in Trello.
Trello is my personal assistant/course coordinator.
I knew online courses had a high drop out rate. I wasn’t going to let myself be a part of this number. I had a mission.
To make myself accountable, I started sharing my learning journey online. I figured I could practice communicating what I learned plus find other people who were interested in the same things I was. My friends still think I’m an alien when I go on one of my AI escapades.
The curriculum has changed slightly since I first wrote it but it’s still relevant and I visit the Trello board multiple times per week to track my progress.
Getting a job
I bought a plane ticket to the US with no return flight. I’d been studying for a year and I figured it was about time I started putting my skills into practice.
My plan was to rock up to the US and get hired.
Then Ashlee messaged me on LinkedIn, “Hey I’ve seen your posts and they’re really cool, I think you should meet Mike.”
I met Mike.
I told him my story of learning online, how I loved healthtech and my plans to go to the US.
“You may be better off staying here a year or so and seeing what you can find, I’ think you’d love to meet Cameron.”
I met Cameron.
We had a similar chat what Mike and I talked about. Health, tech, online learning, US.
“We’re working on some health problems, why don’t you come in on Thursday?”
Thursday came. I was nervous. But someone once told me being nervous is the same as being excited. I flipped to being excited.
I spent the day meeting the Max Kelsen team and the problems they were working on.
Two Thursday’s later, Nick, the CEO, Athon, lead machine learning engineer, and I went for coffee.
“How would you like to join the team?” Asked Nick.
“Sure.” I said.
So it turns out, my US flight got pushed back a couple months and now I’ve got a return ticket.
Sharing your work
Learning online, I knew it was unconventional. All the roles I’d gone to apply for had Masters Degree requirements or at least some kind of technical degree.
I didn’t have either of these. But I did have the skills I’d gathered from a plethora of online courses.
Along the way, I was sharing my work online. My GitHub contained all the projects I’d done, my LinkedIn was stacked out and I’d practiced communicating what I learned through YouTube and articles on Medium.
I never handed in a resume for Max Kelsen. “We checked you out on LinkedIn.”
My body of work was my resume.
Regardless if you’re learning online or through a Masters Degree, having a portfolio of what you’ve worked on is a great way to build skin in the game.
ML and AI skills are in demand but that doesn’t mean you don’t have to showcase them. Even the best product won’t sell without any shelf space.
Whether it be GitHub, Kaggle, LinkedIn or a blog, have somewhere where people can find you. Plus, having your own corner of the internet is great fun.
How do you start?
Where do you go to learn these skills? What courses are the best?
There’s no best answer. Everyone’s path will be different. Some people learn better with books, others learn better through videos.
What’s more important than how you start is why you start.
Start with why.
Why do you want to learn these skills?
Do you want to make money?
Do you want to build things?
Do you want to make a difference?
Again, no right reason. All are valid in their own way.
Start with why because having a why is more important than how. Having a why means when it gets hard and it will get hard, you’ve got something to turn to. Something to remind you why you started.
They’re all world class. I’m a visual learner. I learn better seeing things being done/explained to me on. So all of these courses reflect that.
If you’re an absolute beginner, start with some introductory Python courses and when you’re a bit more confident, move into data science, machine learning and AI.
How much math?
The highest level of math education I’ve had was in high school. The rest I’ve learned through Khan Academy as I’ve needed it.
There are many different opinions on how much math you need to know to get into machine learning and AI. I’ll share mine.
If you want to apply machine learning and AI techniques to a problem, you don’t necessarily need an in-depth understanding of the math to get a good result. Libraries such as TensorFlow and PyTorch allow someone with a bit of Python experience to build state of the art models whilst the math is taken care of behind the scenes.
If you’re looking to get deep into machine learning and AI research, through means of a PhD program or something similar, having an in-depth knowledge of the math is paramount.
In my case, I’m not looking to dive deep into the math and improve an algorithm’s performance by 10%. I’ll leave that to people smarter than me.
Instead, I’m more than happy to use the libraries available to me and manipulate them to help solve problems as I see fit.
What does a machine learning engineer actually do?
What a machine engineer does in practice might not be what you think.
Despite the cover photos of many online articles, it doesn’t always involve working with robots that have red eyes.
Here are a few questions an ML engineer has to ask themselves daily.
Context — How can ML be used to help learn more about your problem?
Data — Do you need more data? What form does it need to be in? What do you do when data is missing?
Modeling — Which model should you use? Does it work too well on the data (overfitting)? Or why doesn’t it work very well (underfitting)?
Production — How can you take your model to production? Should it be an online model or should it be updated at time intervals?
Ongoing — What happens if your model breaks? How do you improve it with more data? Is there a better way of doing things?
I borrowed these from a great article by Rachel Thomas, one of the co-founders of fast.ai, she goes into more depth in the full text.
For more, I made a video of what we usually get up to on Monday’s at Max Kelsen.
No set path
There’s no right or wrong way to get into ML or AI.
The beautiful thing about this field is we have access to some of the best technologies in the world, all we’ve got to do is learn how to use them.
You could begin by learning Python code.
You could begin by studying calculus and statistics.
You could begin by learning about the philosophy of decision making.
Machine learning and AI fascinates me because of this intersection of fields.
The more I learn about it, the more I realise there’s plenty more to learn. And this hypes me up.
Sometimes I get frustrated when my code doesn’t run. Or I don’t understand a concept. So I give up temporarily. I give up by letting myself walk away from the problem and take a nap. Or go for a walk. When I come back it feels like I’m looking at it with different eyes. The excitement comes back. I keep learning.
There’s so much happening in the field it can be daunting to get started. Too many options lead to no options. Ignore this.
Start wherever interests you most and follow it. If it leads to a dead end, great, you’ve figured out what you’re not interested in. Retrace your steps and take the other fork in the road instead.
Computers are smart but they still can’t learn on their own. They need your help.
PS if you want have any questions, feel free to reach out to me anytime at mrdbourke.com.
For his book Photography Changes Everything, Marvin Heiferman spoke to experts in 3-D graphics, neurobiology, online dating, the commercial flower industry, global terrorism, giant pandas, and snowflake structure to understand the infinite ways imagery affects our everyday lives.
Over the last several years, doctors noticed a mystifying trend: Fewer and fewer new pain drugs were getting through double-blind placebo control trials, the gold standard for testing a drug’s effectiveness.
Over the last several years, doctors noticed a mystifying trend: Fewer and fewer new pain drugs were getting through double-blind placebo control trials, the gold standard for testing a drug’s effectiveness.
In these trials, neither doctors nor patients know who is on the active drug and who is taking an inert pill. At the end of the trial, the two groups are compared. If those who actually took the drug report significantly greater improvement than those on placebo, then it’s worth prescribing.
When researchers started looking closely at pain-drug clinical trials, they found that an average of 27 percent of patients in 1996 reported pain reduction from a new drug compared to placebo. In 2013, it was 9 percent.
What this showed was not that the drugs were getting worse, but that “the placebo response is growing bigger over time,” but only in the US, explains Jeffrey Mogil, the McGill University pain researcher who co-discovered the trend. And it’s not just growing stronger in pain medicine. Placebos are growing in strength in antidepressants and anti-psychotic studies as well.
“The placebo effect is the most interesting phenomenon in all of science,” Mogil says. “It’s at the precise interface of biology and psychology,” and is subject to everything from the drug ads we see to our interactions with health care providers to the length of a clinical trial.
Scientists have been studying this incredibly complex interface in great detail over the past 15 years, and they’re finding that sugar pills are stranger and more useful than we’ve previously imagined. The new science of placebo is bringing new understanding to why alternative treatments — like acupuncture and reiki — help some people. And it could also potentially allow us to one day prescribe smaller doses of pain drugs to help address the opioid crisis currently ravaging America.
Most instructively, the science finds that since we can’t separate a medicine from the placebo effect, shouldn’t we use it to our advantage?
There is no one placebo response. It’s a family of overlapping psychological phenomena.
Belief is the oldest medicine known to man.
For millennia, doctors, caregivers, and healers had known that sham treatments made for happy customers. Thomas Jefferson himself marveled at the genius behind the placebo. “One of the most successful physicians I have ever known has assured me that he used more bread pills, drops of colored water, powders of hickory ashes than of all other medicines put together,” Jefferson wrote in 1807. “It was certainly a pious fraud.”
These days, placebo — Latin for “I shall please” — is much more than a pious fraud.
As Ted Kaptchuk at Harvard, who is regarded as one of the world’s leading experts on placebo, put it to me in a recent interview, the study of the placebo effect is about “finding out what is it that’s usually not paid attention to in medicine — the intangible that we often forget when we rely on good drugs and procedures. The placebo effect is a surrogate marker for everything that surrounds a pill. And that includes rituals, symbols, doctor-patient encounters.”
And it’s not just one thing. “I see the placebo effect as a kind of loose family of different phenomena that are just yoked together by this term,” says Franklin Miller, a retired NIH bioethicist who has edited a volume on the subject. “Sooner or later we’ll get rid of the term,” he says, and talk more specifically about each of its components.
The family of placebo effects ranges from the common sense to some head scratchers. Let’s start off with the simplest.
1) Regression to the mean
When people first go to a doctor or start on a clinical trial, their symptoms might be particularly bad (why else would they have sought treatment?). But in the natural course of an illness, symptoms may get better all on their own. In depression clinical studies, for instance, researchers find around one-third of patients get better without drugs or placebo. In other words, time itself is a kind of placebo that heals.
Sugar pills and active drugs can both change the way patients report symptoms.
2) Confirmation bias
A patient may hope to get better when they’re in treatment, so they will change their focus. They’ll pay closer attention to signs that they’re getting better and ignore signs that they’re getting worse. (Relatedly, there’s theHawthorne effect: We change our behavior when we know we’re being watched.)
But as we’ve seen, the placebo effect is more than just bias. There’s also:
3)Expectations and learning
The placebo response is something we learn via cause and effect. When we take an active drug, we often feel better. That’s a memory we revisit and recreate when on placebo.
Luana Colloca, a physician and researcher at University of Maryland, has conducted a number of studies on this phenomenon. And they typically go like this: She’ll often hook up a study participant to an electroshock machine. For each strong, painful shock, she’ll flash a red light on a screen the participant is looking at. For mild shocks, she’ll flash a green light. By the end of the experiment, when the participants see the green light, they feel less pain, even when the shocks are set to the highest setting.
The lesson: We get cues about how we should respond to pain — and medicine — from our environments.
Take morphine, a powerful drug that acts directly on neurochemical receptors in the brain. You can become addicted to it. But its analgesic powers grow when we know we’re taking it, and know a caring professional is giving it to us.
Studies show that post-operative patients whose painkillers are distributed by a hidden robot pump at an undisclosed time need twice as much drug to get the same pain-relieving effect as when the drug is injected by a nurse they could see. So awareness that you’re being given something that’s supposed to relieve pain seems to impact perception of it working.
Pain relief is stronger and more immediate when morphine is injected out in the open.The Lancet Neurology
The research also suggests that fake surgeries — where doctors make some incisions but don’t actually change anything — are an even stronger placebo than pills. A 2014 systematic reviewof surgery placebos found that the fake surgery led to improvements 75 percent of the time. In the case of surgeries to relieve pain, one meta-review found essentially no difference in outcomes between the real surgeries and the fake ones.
There is such thing as the nocebo effect: where negative expectations make people feel worse. Some researchers think this is what’s fueling the gluten-free diet fad. People have developed a negative expectation that eating gluten will make them feel bad. And so it does, even though they may not have any biological gluten sensitivity.
4) Pharmacological conditioning
This is where things get a little weird.
Colloca has conducted many studies where for several days, a patient will be on a drug to combat pain or deal with the symptoms of Parkinson’s disease. Then one day, she’ll surreptitiously switch the patient over to a placebo. And lo and behold, they still feel healing effects.
On that fifth day, it seems the placebo triggers a similar response in the brain as the real drug. “You can see brain locations associated with chronic pain and chronic psychiatric disease” acting like there are drugs in the system, she says. For instance, Colloca has found that individual neurons in the brains of patients with Parkinson’s disease will still respond to placebos as though they are actual anti-Parkinson’s drugs after such conditioning has taken place.
The brain can learn to associate taking a pill with relief, and produce the same brain chemicals when drug is replaced with placebo.
What’s going on here? Learning. Just like Pavlov’s dogs learned to associate the sound of a bell with food and would start to salivate in anticipation, our brains learn to associate taking a pill with relief, and start to produce the brain chemicals to kick-start that relief.
This pharmacological conditioning only works if the drug is acting on a process that the brain can do naturally. “You can condition pain relief because there are endogenous pain-relieving mechanisms,” Miller says. Painkillers activate the opioid system in the brain. Taking a pill you think is a painkiller can activate that system (to a lesser degree).
And some studies do suggest that the placebo effect’s powers may possibly move beyond the brain.
Researchers have used flavored drinks to condition an immune response to placebo.
In a 2012 study, participants were given a sweet drink along with a pill that contained an immune suppressant drug for a few days. Without notice, the drug was swapped with placebo on one of the trial days. And their bodies still showed a decreased immune response. Their bodies had learned to associate the sweet drink with decreased production of interleukin, a key protein in our immune systems, which is produced in many cells outside the brain.
Results like these show “we are talking about a neurobiological phenomenon,” Colloca says.
5) Social learning
When study participants see another patient get relief from a placebo treatment (like in the electroshock experiment described above), they have a greater placebo response when they’re hooked up to the machine.
6) A human connection
Irritable bowel syndrome is an incredibly hard condition to treat. People with it live with debilitating stomach cramps, and there are few effective treatments. And doctors aren’t sure of the underlying biological cause.
It’s the type of ailment that’s sometimes derided as “all in their head,” or a diagnosis given when all others fail. In the early 2000s, Harvard’s Ted Kaptchuk and colleagues conducted an experiment to see if usually intangible traits like warmth and empathy help make patients feel better.
In the experiment, 260 participants were split into three groups. One group received sham acupuncture from a practitioner who took extra time asking the patient about their life and struggles. He or she took pains to say things like, “I can understand how difficult IBS must be for you.” A second group got sham acupuncture from a practitioner who did minimal talking. A third group was just put on a waiting list for treatment.
A caring provider can create a stronger placebo response than an apathetic one.
The warm, friendly acupuncturist was able to produce better relief of symptoms. “These results indicate that such factors as warmth, empathy, duration of interaction, and the communication of positive expectation might indeed significantly affect clinical outcome,” the study concluded.
Participants in the “augmented” condition — the one in which the caregivers were extra attentive — reported better outcomes at the end of the three-week trial, compared with both participants who received treatment as normal and those waiting for treatment.BMJ
This may be the least-understood component of placebo: It’s not just about pills. It’s about the environment a pill is taken in. It’s about the person who gave it to you — and the rituals and encounters associated with them.
What placebos can, and can’t,do
Placebos seem to have the greatest power over symptoms that lie at the murky boundary between the physical and psychological.
A 2010 systematic review looked at 202 drug trials where a placebo group was compared to patients who received neither placebo nor active drug. And it found that placebos seem to move the needle on pain, nausea, asthma, and phobias, with more inconsistent results for outcomes like smoking, dementia, depression*, obesity, hypertension, insomnia, and anxiety. (*Separate literature review on depression meds doesfind an effect of placebo compared with no treatment.)
“It seems like placebo taps into a family of psychological and brain processes that’s very much something we evolved for,” says Tor Wager, a University of Colorado Boulder neuroscientist who has co-authored many of the key papers on the neuroscience of placebo. “Take pain as an example. If you step on something sharp, there’s pain in your foot. Now, how should you respond to it? Well, if you are running from an attack, you don’t even want to feel that. You keep going.”
Another way to think about it: Placebos tweak our experience of symptoms, not their underlying causes.
A 2011 study elegantly illustrates this. In the experiment, asthma patients were randomly sorted into three groups: One group received an inhaler with albuterol, a drug that opens the airways. Another group got an inhaler with a placebo. A third group got “sham” acupuncture (meaning the needles were withdrawn before they touched the skin). A fourth got nothing. The study authors evaluated lung function on two metrics: self-report from the patients on their asthma symptoms, and an objective measure of lung functioning.
If you go by self-report, it looks like the placebo, albuterol, and sham acupuncture are all equally effective.
The objective measure, however, shows only the albuterol improved airflow. (FEV is a measure of lung function.)
Which isn’t to say that the self-reported improvement on placebo doesn’t matter. In many illnesses, patients would love a greater opportunity to ignore their symptoms.
“In all the objectively measurable illnesses, like cancer, even heart disease, there are components of it that are not [objectively measurable],” Kaptchuk says. And it’s those symptoms that are the prime targets to treat with placebo.
Placebo can only help symptoms that can be modulated by the mind. “There are real limits to what you can condition,” Miller says. You can’t, for example, condition the cancer-killing effects of chemotherapy. Our bodies don’t produce cancer-killing chemicals.
There’s evidence that placebos actually release opioids in the brain
Over the past 15 years, scientists have made some of their most interesting discoveries looking at how placebos have a powerful impact on the brain.
“When I first started studying placebo effects, it kind of seemed like magic — for some reason, your brain mimicked a drug response,” Wager says. “The biggest change in this field in the last 15 years is that neuroscientists are beginning to uncover the underlying neural mechanisms that create the placebo response.”
Placebos, researchers have found, actually prompt the release of opioids and other endorphins (chemicals that reduce pain) in the brain. Other findings:
Drugs that negate the effects of opioids — such as naloxone— also counteract the placebo effect, which shows that placebos are indeed playing on the brain’s natural pain management circuitry.
The periaqueductal gray matter, a region of the brain key for pain management, shows increased activity under placebo. Regions of the spinal cord that respond to pain show decreased activity under placebo, which suggests either the sensation of pain or our perception of it is diminished under placebo.
Patients with Alzheimer’s disease start to show a diminished placebo response. It’s probably due to the degradation of their frontal lobes, the area of the brain that helps direct our subjective experience of the world.
Our understanding of all this is far from complete, Wager says. For one, researchers still don’t completely understand how the brain processes pain. A lot of the brain regions implicated in the placebo response also play a role in emotions. So we don’t yet know if placebo is actually reducing our sensation of pain, or just our interpretation of it. (Also, as with a lot of neuroscience studies, a brain area might “light up” in an experiment, but it’s really, really hard to know what exactly is going on.)
“So really, what we should be concluding from those studies is something like ‘placebo affects the pain you report,’” Wager says. “What does pain mean to you? That’s a decision that’s made in your brain in different circuits, and that’s essential to placebo.”
You can tell people they’re taking a sugar pill for their illness, and they’ll still feel better
Kaptchuk has studied the placebo effect for decades, and something always bothered him: deception. Placebo studies have long relied on double-blind procedures. It ensures scientific rigor but keeps patients in the dark about what they’re actually taking.
“About five years ago, I said to myself, ‘I’m really tired [of] doing research that people say is about deception and tricking people,’” he says.
So he wanted to see: Could he induce a placebo response even when he told patients they were on placebo?
His own randomized controlled trials found that giving patients open-label placebos — sugar pills that the doctors admit are sugar pills — improved symptoms of certain chronic conditions that are among the hardest for doctors to treat, including irritable bowel syndrome and lower back pain. And he wonders if chronic fatigue — a hard-to-define, hard-to-treat, but still debilitating condition — will be a good future target for this research.
“Our patients tell us it’s nuts,” he says. “The doctors think it’s nuts. And we just do it. And we’ve been getting good results.”
Kaptchuk’s work adds a few new mysteries to the placebo effect. For one, he says that the placebo effect doesn’t require patient expectations for a positive outcome to work. “All my patients are people who have been to many doctors before. They don’t have positive expectations about getting better,” he says. “They’ve been to 10 doctors already.”
Colloca has a different interpretation of his results. She says there’s a difference between belief and expectation, so while the patients may not believe the pill will work, they still unconsciously expect it to.
That’s because, she says, they still have a deep-seated conditioned memory for what it means to take a pill. They have a conditioned memory for what it means to be in the care of another person. And that memory is indeedan expectation that can kick-start the analgesic effect in the brain. They don’t have to be aware it’s happening.
Some doctors wonder if placebos can be integrated into mainstream medicine
The researchers I spoke to for this story are overall optimistic that these discoveries can be used in the clinical settings. There’s a lot of work left to do here, and certainly some of the findings are easier to implement than others. For instance, we could start with reminding doctors that they can relieve pain simply by being warm and caring to their patients.
Colloca wonders if the placebo effect can also be harnessed so that the millions living with chronic pain can feel the same therapeutic effects with a lower dosage of opioid treatments that are both ineffective and deadly.
The NIH’s Miller says it’s too soon to start prescribing placebos, or using the effect, to decrease the dosage of a drug. For one, most of these studies are short-term and conducted with healthy volunteers, not actual patients.
“There’s still lot we don’t know,” he says. Like side effects: Just as a placebo can mimic a drug, it can also mimic a side effect. “We haven’t done the kinds of studies that will indicate that you can maintain therapeutic benefit at lower side effect burden.”
More broadly, Kaptchuk says, for years researchers have seen the placebo as a hurdle to clear to produce good medicine. But placebo is not just a hurdle. “It’s basically the water that medicine swims in,” he says. “I would like to see the bottom line of my research change the art of medicine into the science of medicine.”


/arc-anglerfish-tgam-prod-tgam.s3.amazonaws.com/public/KZEZQXKH25HGXDAIW6Z76IFH6Q.jpg)


/cdn.vox-cdn.com/uploads/chorus_image/image/55606685/PLACEBO_LEAD.0.jpg)
:format(webp)/cdn.vox-cdn.com/uploads/chorus_asset/file/8803615/500PX_500PX.jpg)
:format(webp)/cdn.vox-cdn.com/uploads/chorus_asset/file/8803597/500PX_500PX_copy_3.jpg)
:format(webp)/cdn.vox-cdn.com/uploads/chorus_asset/file/8732863/Screen_Shot_2017_06_22_at_12.11.19_PM.png)
:format(webp)/cdn.vox-cdn.com/uploads/chorus_asset/file/8803589/500PX_500PX_copy.jpg)
:format(webp)/cdn.vox-cdn.com/uploads/chorus_asset/file/8803653/drink.jpg)
:format(webp)/cdn.vox-cdn.com/uploads/chorus_asset/file/8803735/acupuncture.jpg)
:format(webp)/cdn.vox-cdn.com/uploads/chorus_asset/file/8806627/Screen_Shot_2017_07_06_at_9.48.01_AM.png)
:format(webp)/cdn.vox-cdn.com/uploads/chorus_asset/file/8719553/mindfulness_chart1.jpg)
:format(webp)/cdn.vox-cdn.com/uploads/chorus_asset/file/8719547/mindfulness_chart2.jpg)